Managing patients with multiple failed surgical heart valves is one of the most challenging areas in modern cardiology. Redo open-heart surgery carries very high risk, especially in elderly patients with prior infections and multiple previous valve replacements.
Advances in transcatheter valve therapies now allow such complex cases to be treated minimally invasively, offering hope where surgery may not be feasible.
This blog explains a rare and advanced combined transcatheter procedure—TAVI (Transcatheter Aortic Valve Implantation) and TMVR (Transcatheter Mitral Valve Replacement)—performed in a single patient with multiple prior valve surgeries.
Patient Background
A 74-year-old male presented with progressive breathlessness, worsening from NYHA Class II to Class III over one year, significantly limiting daily activities.
Past Cardiac History
-
Rheumatic heart disease
-
Severe mitral regurgitation with infective endocarditis
-
Mild aortic stenosis
Previous Surgeries
-
2004: Mitral Valve Replacement (MVR) with 29-mm Omnicarbon mechanical valve
-
2007:
-
Redo mitral valve replacement using Edwards pericardial tissue valve
-
Aortic valve replacement with 23-mm Edwards Perimount bioprosthetic valve
-
-
History of recurrent endocarditis involving prosthetic mitral, native aortic, and tricuspid valves
Given multiple prior sternotomies and infections, the patient was considered extremely high risk for repeat open-heart surgery.
Current Evaluation
Echocardiography Findings
-
Severe Mitral Stenosis (MS) due to degenerated surgical mitral bioprosthesis
-
Severe Aortic Stenosis (AS) of the surgical aortic valve
-
Elevated filling pressures explaining progressive heart failure symptoms
A heart team discussion (interventional cardiology, cardiac surgery, imaging, and anesthesia) concluded that a combined transcatheter approach was the safest and most effective option.
Why a Combined TAVI + TMVR Approach?
Redo surgical replacement of both aortic and mitral valves would involve:
-
Very high operative mortality
-
Prolonged recovery
-
Increased risk of bleeding and infection
A transcatheter valve-in-valve strategy allows:
-
Treatment without reopening the chest
-
Faster recovery
-
Lower procedural risk
-
Preservation of existing surgical valve frames
Step-by-Step Procedure Explanation
1. Transcatheter Aortic Valve Implantation (TAVI)
-
A 23-mm Myval transcatheter heart valve was implanted inside the degenerated surgical aortic bioprosthesis
-
This restored normal aortic valve opening and relieved the obstruction
-
Proper positioning and expansion were confirmed fluoroscopically
2. Balloon Valve Fracture of Surgical Aortic Valve
-
A 24 × 40 mm Atlas Gold balloon was used
-
High-pressure balloon inflation fractured the rigid surgical valve ring
-
This step:
-
Improved valve expansion
-
Reduced residual gradients
-
Optimized long-term valve performance
-
3. Transseptal Access for TMVR
-
A septal puncture was performed to access the left atrium
-
Left atrial entry was carefully confirmed
-
Atrial septal dilation was done to allow safe passage of large delivery systems
4. Crossing the Surgical Mitral Valve
-
The degenerated surgical mitral valve was crossed using a pigtail catheter through an Agilis sheath
-
This step is technically demanding due to altered anatomy from previous surgeries
5. Transcatheter Mitral Valve Replacement (TMVR)
-
A 29-mm Myval transcatheter valve was advanced across the surgical mitral valve
-
Precise positioning was achieved under fluoroscopic guidance
-
The valve was successfully deployed, restoring mitral valve function
6. Balloon Valve Fracture of Surgical Mitral Valve
-
Balloon valve fracture was again performed
-
This ensured:
-
Full valve expansion
-
Optimal leaflet motion
-
Lower transmitral gradients
-
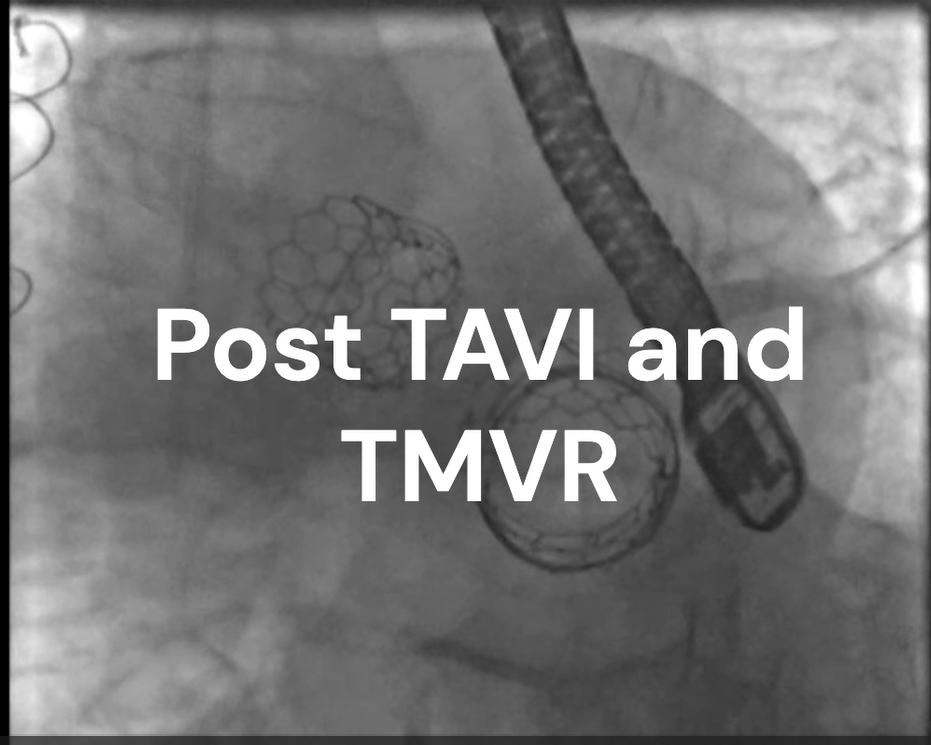
Final Outcome
-
Both aortic and mitral valves were successfully treated
-
Final imaging showed:
-
Well-seated transcatheter valves
-
No significant paravalvular leak
-
Marked reduction in valve gradients
-
-
The patient showed clinical improvement in symptoms
This case highlights how advanced transcatheter techniques can safely manage even the most complex valve failures.
Why This Case Is Important
-
Demonstrates feasibility of dual valve-in-valve therapy
-
Avoids high-risk redo open-heart surgery
-
Requires:
-
Advanced imaging
-
Precise procedural planning
-
High operator expertise
-
Such procedures should only be performed at experienced structural heart centers.
Frequently Asked Questions (FAQs)
1. What is valve-in-valve therapy?
Valve-in-valve therapy involves placing a new transcatheter valve inside a failing surgical valve, avoiding the need for open surgery.
2. Is it safe to replace two valves in one procedure?
Yes, in selected high-risk patients, combined TAVI and TMVR can be safely performed by experienced teams with careful planning.
3. What is balloon valve fracture and why is it needed?
Balloon valve fracture uses high-pressure balloons to break the rigid surgical valve frame, allowing:
-
Better expansion of the new valve
-
Lower pressure gradients
-
Improved long-term outcomes
4. How long is recovery after TAVI and TMVR?
Most patients recover much faster than with open surgery, often walking within 24–48 hours and discharged in a few days.
5. Who is eligible for TMVR and TAVI?
Typically:
-
Elderly patients
-
Patients with prior valve surgery
-
High surgical risk patients
Eligibility is determined by a multidisciplinary heart team.
6. Are these valves durable?
Current data shows excellent short- and mid-term durability, and outcomes continue to improve with newer valve designs.
—————————————————————-
Dr. Rajasekar V
Senior Interventional Cardiologist
Expert in Structural Heart Interventions, including:
-
TAVI / TAVR
-
TMVR
-
Valve-in-Valve procedures
-
Complex high-risk structural heart cases
With extensive experience in managing redo valve failures and advanced transcatheter therapies, Dr. Rajasekar V specializes in offering minimally invasive solutions for patients deemed high risk for surgery.